
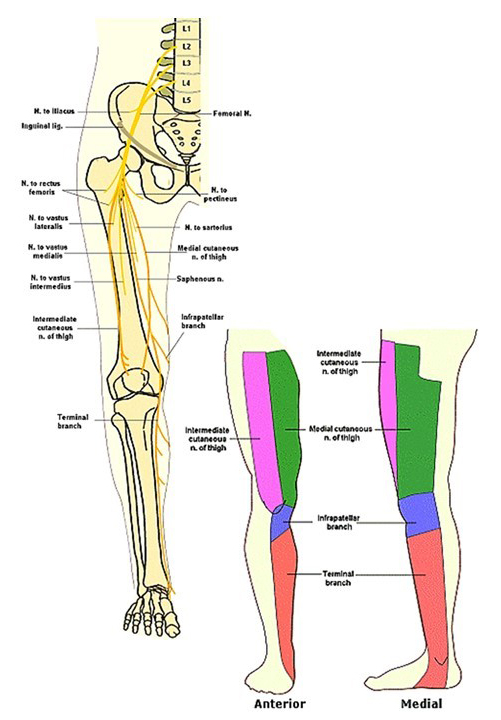
Femoral Nerve
There are three main nerves in the thigh—the femoral nerve, the obturator nerve, and the sciatic nerve. This diagram shows the distribution of the femoral nerve.
The femoral nerve arises from the second, third, and fourth lumbar spinal nerves and enters into the pelvis where it gives innervation to the psoas major and the iliacus, which are two main hip flexors. It then passes into the anterior thigh, going to the quadriceps muscles and sending off cutaneous branches to the anterior of the thigh. One of these branches, called the saphenous nerve, continues down the medial aspect of the leg and into the ankle, providing sensory distribution to those areas from the femoral nerve.
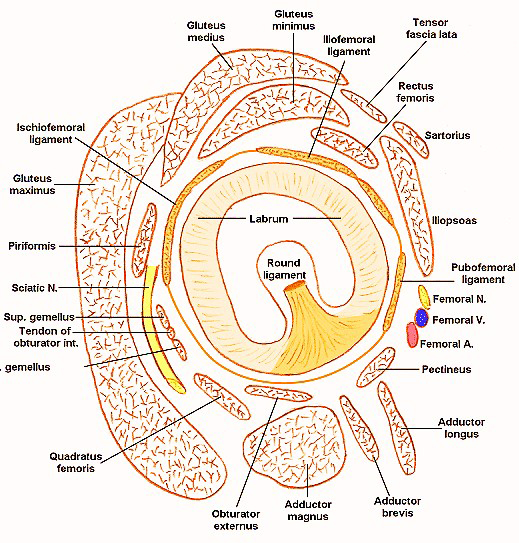
Hip Joint
This is a view of the hip joint with the head of the femur removed looking down at the acetabulum. You can see that the acetabulum is deepened by the acetabular labrum, and that, at the bottom, where the acetabular notch is, there is a ligament called the transverse acetabular ligament.
Rising from that ligament is the round ligament of the femur. The round ligament contains blood supply to the head of the femur. And if it is disrupted, you end up with necrosis of the femoral head.
The joint capsule surrounding the hip joint has three thickenings, and these are the two anterior ligaments of the hip joint—the iliofemoral ligament and the pubofemoral ligament. Posteriorly is the ischiofemoral ligament.
The hip joint is surrounded by musculature. On the back are the gluteal muscles. In front, are the hip flexors and the femoral blood vessels and nerves. And then, medially and inferiorly, are the adductors of the hip.
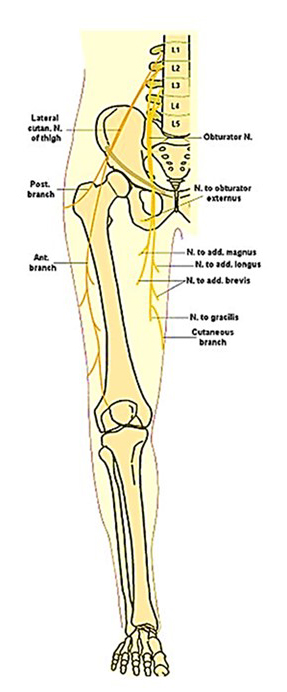
Obturator Nerve
This is a diagram showing the distribution of the obturator nerve. The obturator nerve arises from spinal nerves L2, L3, and L4. It travels down through the pelvis, through the obturator foramen of the pubic bone, and then enters the medial aspect of the thigh. There it gives off motor branches to the adductors of the hip, as well as sensory branches to the medial aspect of thigh.
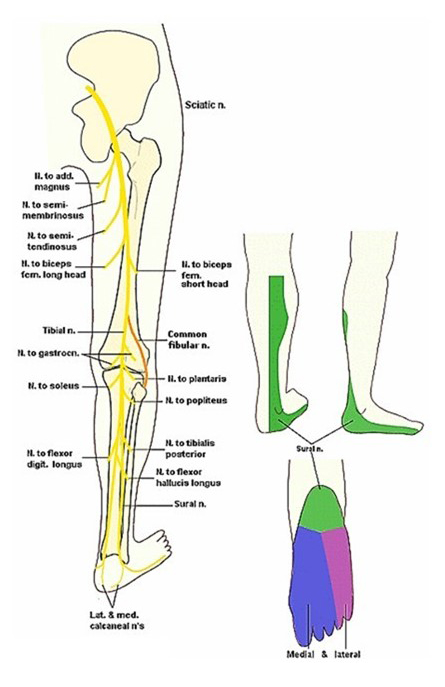
Sciatic Nerve
This is a diagram showing the distribution of the sciatic nerve. The sciatic nerve arises from spinal nerves L4 through S3, and then travels in the pelvis and down the posterior aspect of the thigh. The nerve is actually a combination of two nerves—the tibial nerve and the common fibular nerve.
The tibial owner goes to the adductor magnus and the semimembranosus and tendinosus muscles of the hamstring in the posterior thigh, while the common fibular portion goes to the biceps femoris part of the hamstrings in the posterior thigh. At the area of the popliteal fossa, the tibial and common fibular nerve become separated, and then continue down into the leg and foot.
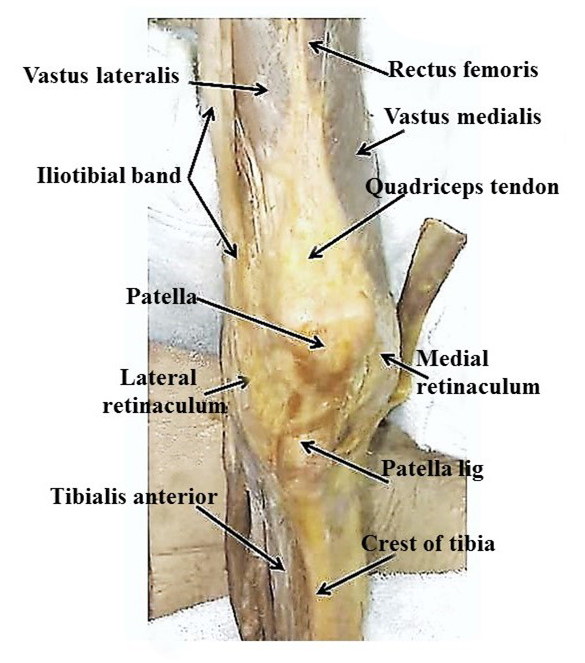
Medial and Lateral Retinaculum
The patellofemoral joint is stabilized by the quadriceps tendon, the patellar ligament, the medial retinaculum, and the lateral ret. The medial retinaculum is formed by the fascia of the vastus medialis muscle, extending onto the medial aspect of the patella. The lateral retinaculum is formed by fascia from the iliotibial band, and the vastus lateralis, combining to form this retinaculum on the lateral side of the patella. The medial and lateral retinacula are also important stabilizing structures for the tibiofemoral joint.
X-Sec of Leg
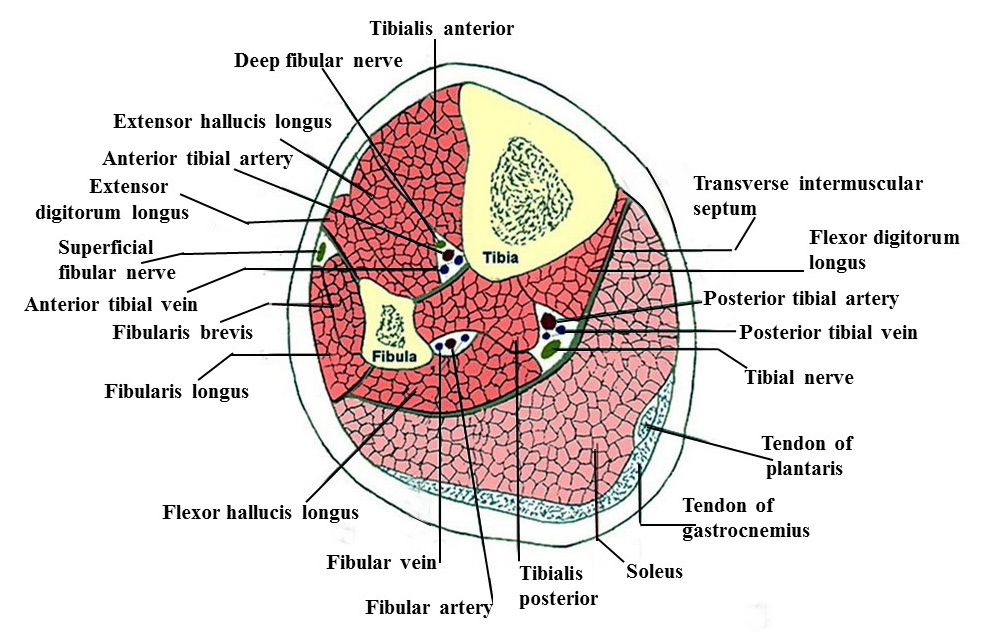
This drawing illustrates the three compartments of the leg. In the upper part of this figure is the anterior compartment. On the left is the lateral compartment. And on the inferior part of this image is the posterior compartment.
The anterior compartment consists of muscles, the dorsal flex, the ankle, and extends to the toes. It contains the anterior tibial artery and the deep fibular nerve.
The lateral compartment contains the everters of the foot—the fibularis longus and brevis, and the superficial fibular nerve.
The posterior compartment contains the plantar flexors of the ankle, the inverters of the foot, and the flexors of the toes. It contains two layers—a superficial layer with clandar flexors and inverters, and a deep layer with flexors of the toes and inverters of the foot.
The posterior compartment also contains the fibular artery, the posterior tibial artery, and the tibial nerve. The posterior tibial artery and the tibial nerve go on to form the plantar arteries and nerves of the foot.
Foot Arteries
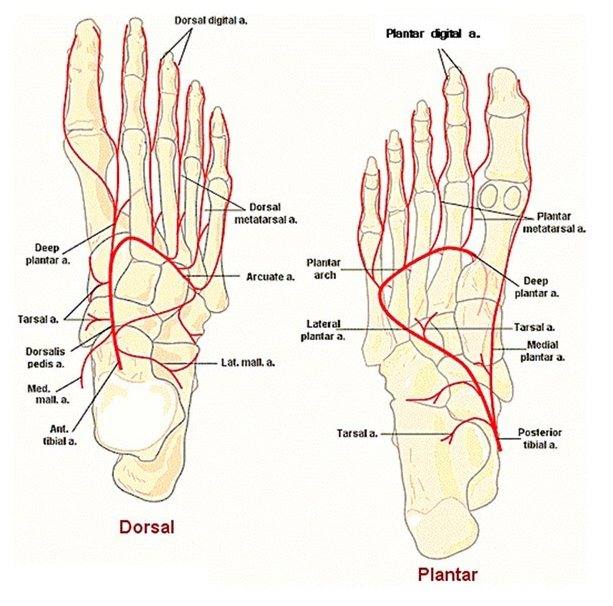
This drawing shows the arteries of the foot. On the left, is a view of the dorsum of the foot. On the right, is a view of the plantar aspect of the foot. If we look at the dorsum of the foot, we see that the anterior tibial artery comes down and, when it crosses the ankle, it changes names into the dorsalis pedis artery. It gives off some malleolar and tarsal arteries, and then forms an arcuate artery and a deep plantar artery.
The deep plantar artery will go between the first and the second metatarsal and enter the plantar surface of the foot, where it will join the plantar arch. Branches off the archway go to form the metacarpal and digital arteries. On the plantar surface of the foot on the right, the posterior tibial artery comes down and divides into a medial and lateral plantar artery.
The medial plantar artery goes pretty much to the big toe, whereas the lateral plantar artery comes around and forms a plantar arch along with the deep plantar artery from the dorsum of the foot. Off of the arch are the plantar metatarsal and digital arteries.
Abdominal Planes
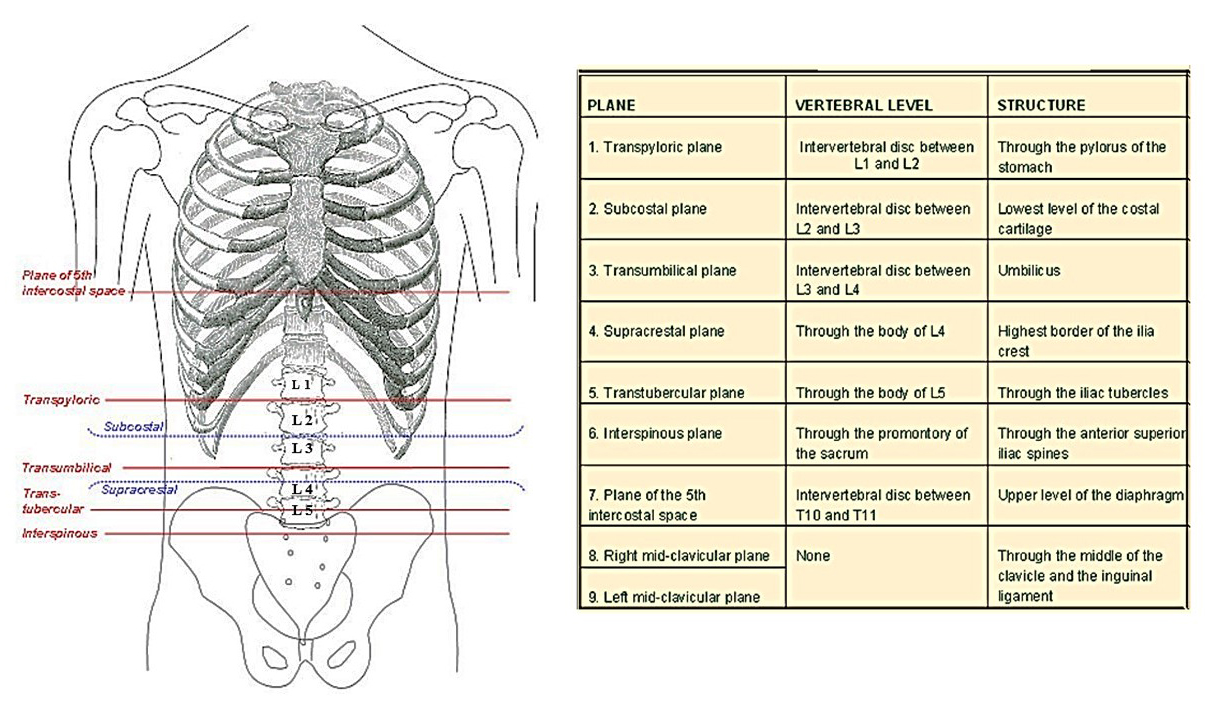
The diagram on your left shows the horizontal planes of the abdomen as they pass through the vertebrae and various organs. The table on your left shows you what organs these planes pass through, as well as the vertebral level where they can be found. These planes are valuable clinically for quickly identifying the levels of the lumbar spine. For example, the transtubercular plane goes through the body of L5, whereas the supracristal plane goes through L4, and the subcostal plane runs between the second and third lumbar vertebrae.
Abdominal Regions
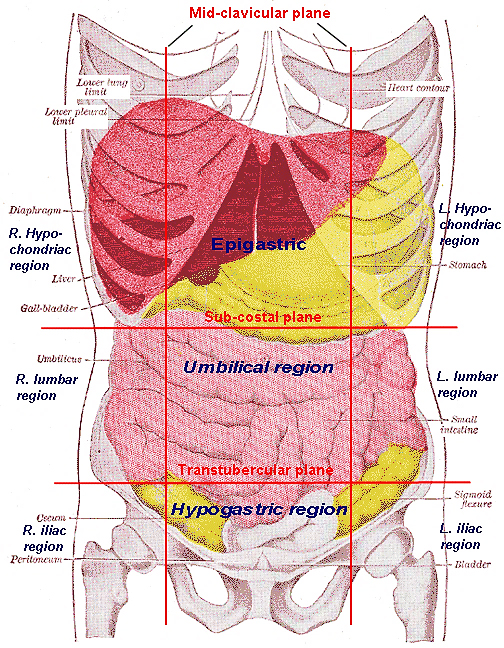
The subcostal and transtubercular plane, and the midclavicular planes, divide the abdomen into nine regions. The upper three regions consist of the epigastric region in the center and the hypochondriac regions on each side. The middle regions are the umbilical, on the center, with the lumbar on each side. The lower three regions are the hypogastric region, in the center, and the iliac regions on each side.
Notice that in each region, there are certain abdominal organs. For example, in the epigastric region, you can see the liver, the gallbladder, and part of the stomach. The pancreas is also in the area, as is part of the transverse colon. Whereby in the left hypochondriac region, we have part of the stomach, which the spleen is underneath. The umbilical region is pretty much small intestines—with the right lumbar being the ascending colon and the left lumbar the descending colon.
The hypogastric region contains the area of the sigmoid colon, the rectum, and the bladder. The right iliac contains the cecum of the large intestine and, the left, also part of the sigmoid colon. Knowing where these organs are relative to the regions is important because there are many referred pain patterns arising from the visceral organs that also refer up and to the shoulder, the back, and other areas where, typically, musculoskeletal problems occur.
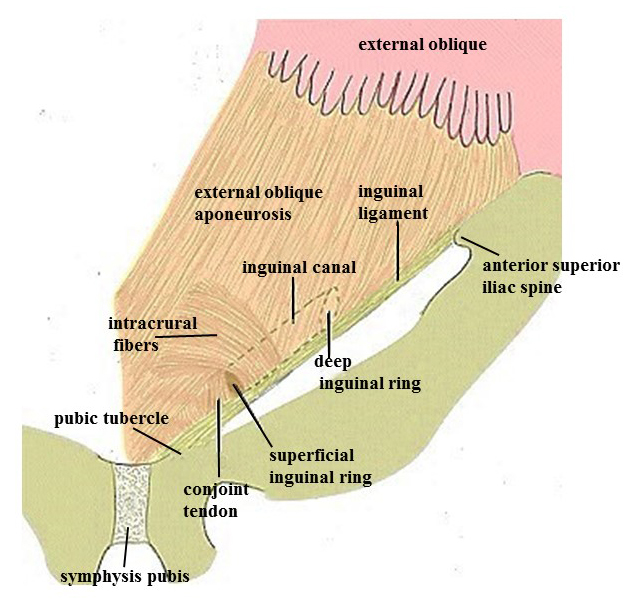
Inguinal Canal
The inguinal ligament is formed by the aponeurosis of the external abdominal oblique muscle and runs from the anterior superior iliac spine to the pubic tubercle. Above the inguinal ligament is the inguinal canal, which connects the abdominal cavity with the superficial abdominal wall.
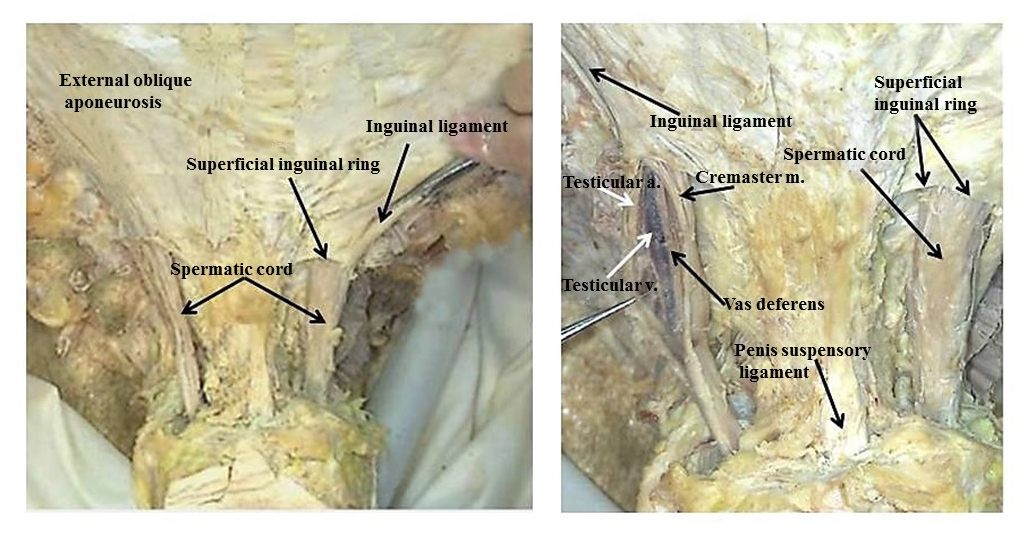
Male Inguinal Contents
This is a dissection of the male inguinal region showing all inguinal ligaments and the superficial inguinal ring which is the outer opening of the inguinal canal. In the male structures that pass through the inguinal canal are the spermatic cord, which contains the testicular artery in vein, the vas deferens, the genital branch of the genitofemoral nerve, and also the ilioinguinal nerve. In the female, the inguinal canal contains the round ligament of the uterus, the genital branch of the genitofemoral nerve, and the ilioinguinal nerve.
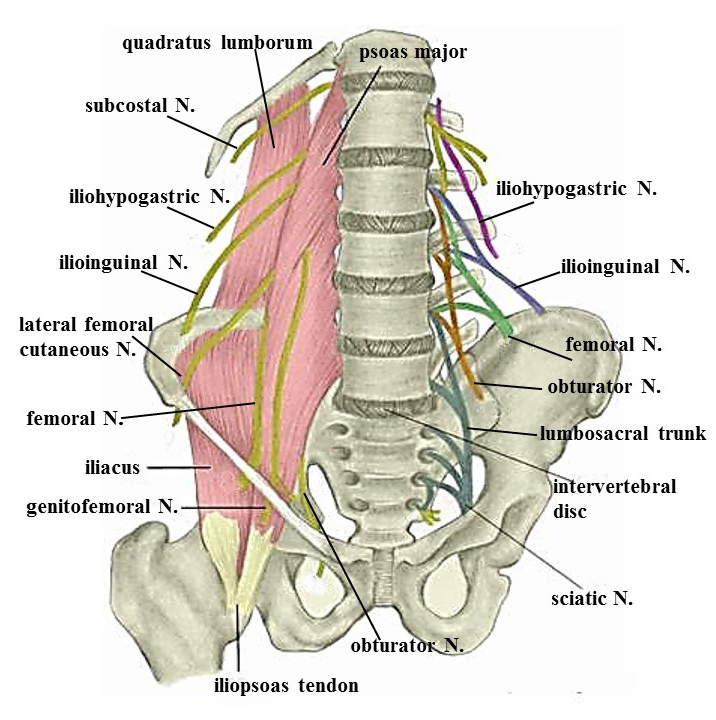
Posterior Abdominal Wall
The posterior wall of the abdomen contains two large muscles—the quadratus lumborum and the psoas major. It also contains the nerves of the lumbar plexus, beginning at the top with the iliohypogastric and then going distally to the ilioinguinal; the lateral femoral cutaneous; and the femoral. Then, coming through the psoas major, is the genitofemoral nerve. And, then, coming medial to it is the obturator nerve. The last part of the lumbar plexus is the lumbosacral trunk, which carries nerve fibers from the L4 and L5 to the sacral plexus.
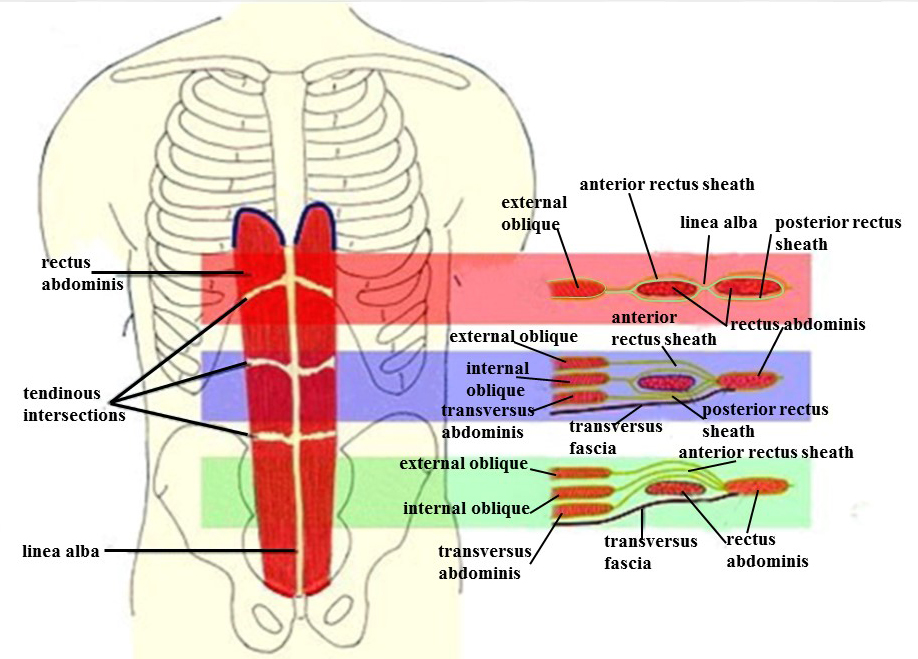
Rectus Sheath
The posterior wall of the abdomen contains two large muscles—the quadratus lumborum and the psoas major. It alsThe rectus abdominis muscle is enveloped in a fiber sheath called the rectus sheath. This sheath is formed by aponeurosis from the lateral abdominal muscles. The arrangement of this sheath, however, varies depending upon the region of the abdomen in the epigastric region. The only muscle there is the external abdominal oblique, and so the anterior and the posterior aspects of the sheath are formed by this muscle.
In the umbilical region, there is now the external oblique, the internal oblique, and the transverse abdominis. Here, the external and internal form the anterior part of the sheath, and the internal and transverse form the posterior part of the sheath. In the hypogastric region, all three lateral abdominal muscles form the anterior part of the sheath, and posteriorly is only a thin fascia, known as the transverse abdominal fascia.
The rectus abdominis fortified by this sheath provides a stabilizing element for the lumbar vertebrae and the trunk. Also, because of the thin posterior sheath in the hypogastric region, this region has less protection against infections from the abdomen than the epigastric or umbilical regions because of the posterior rectus sheath being formed by aponeurosis of the lateral abdominal muscles.
Abdominal Arteries
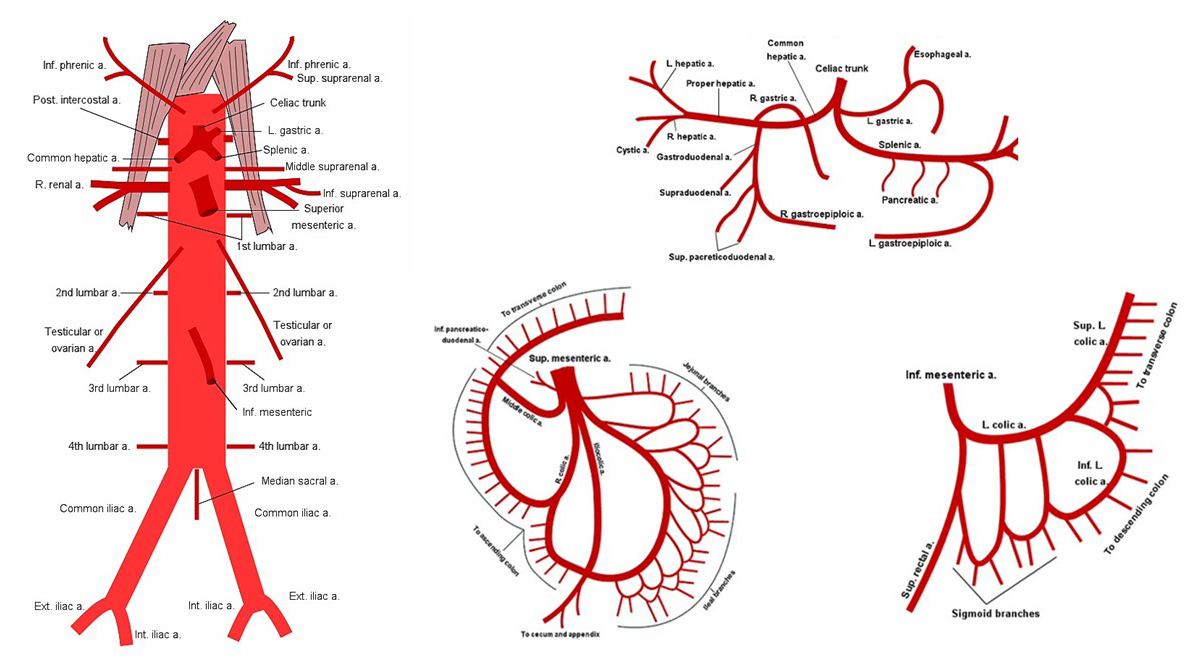
This diagram shows the arteries of the abdomen. Please remember that for each of these arteries there is also a vein accompanying it. Some of these veins go to the portal system and others into the systemic system. The diagram on your left is a look at the entire abdominal aorta showing where the different branches arise from, and the three diagrams on the right are major arteries coming off the aorta.
The top one is the celiac trunk with its three major arteries, the left gastric, the common hepatic, and the splenic. The next one down is the superior mesenteric, with its branches going to the cecum, ascending, and prior transverse colon. And then, to the right of that, is the inferior mesenteric, with its branches going to the part of the transverse colon, the descending colon, and sigmoid colon and rectum.
Kidney
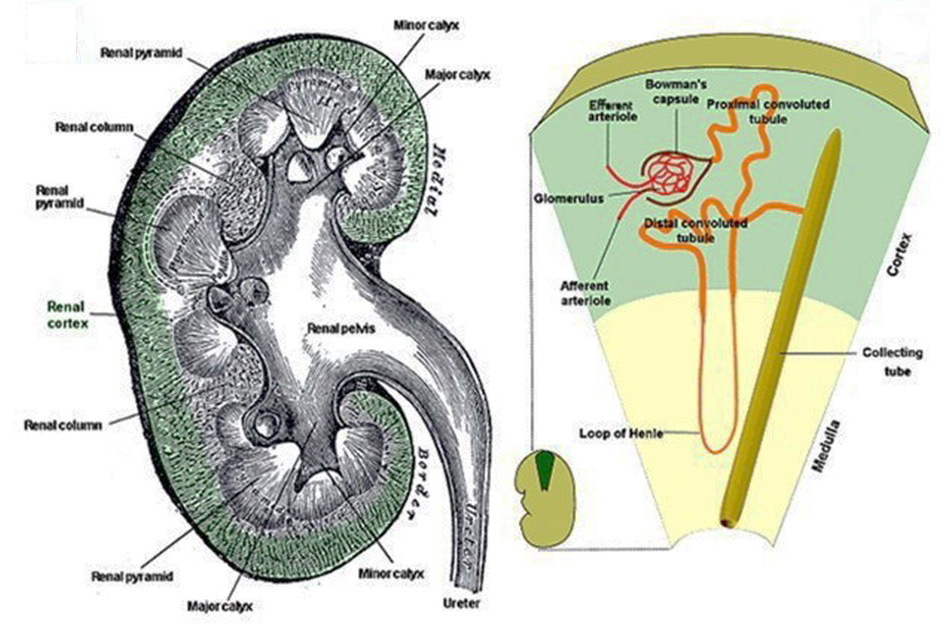
The kidney lies in the upper posterior aspect of the abdominal cavity. It is protected, somewhat, by the ribs and by the quadratus lumborum muscle but, also, by a very heavy renal fat pad. In the drawing on your left, is a longitudinal section through the kidney showing the cortex, the renal pyramids, and the medulla. You can see that in the cortex we have these pyramids that come down into small papilla and then lie in to a funnel. These small funnels are known as the minor calices, and several minor calices that come together form a major calyx. The major calices then go into the renal pelvis, which is continuous with the ureter, which takes the fluids down into the bladder.
On the right, is a diagrammatic drawing of the uriniferous tubule. The uriniferous tubule has two parts. There is the nephron, which is made up of the glomerulus, which is a capillary bed. And that glomerulus is surrounded by a capsule known as Bowman’s capsule. Fluids from the glomerulus are picked up by Bowman’s capsule and passed through a series of tubules.
The first tubule is the proximal convoluted tubule, which goes to the Henle loop and then to the distal convoluted tubule. That makes up the nephron. The distal convoluted tubule then empties into the collecting tube. So the uriniferous tubule consists of two parts, the nephron and the collecting tube.
Portal Vein
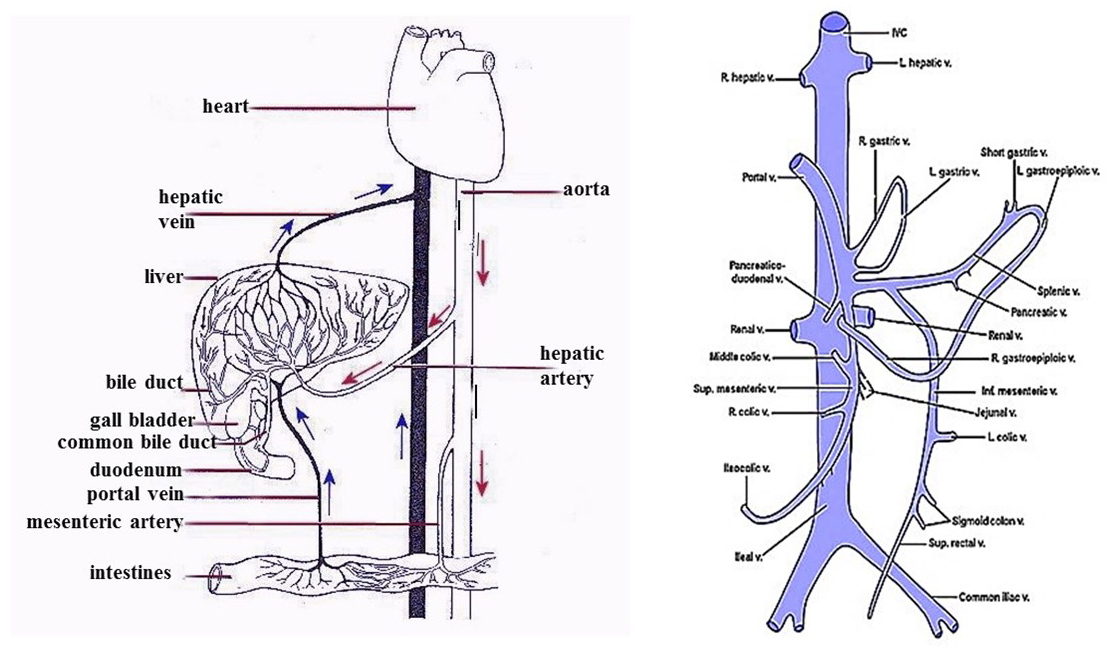
This is a diagram of the hepatic portal system. A portal system begins with a series of capillaries that empty into veins and then empty back into capillaries again. The hepatic portal system begins at the intestines with veins from the digestive system draining into the hepatic portal vein. The hepatic portal vein then goes into the liver where the material is processed, and the processed material goes out of the liver through the hepatic veins and into the inferior vena cava.
The portal vein is made up of two major digestive veins—one is the splenic and the other one is the superior mesenteric vein. All the veins that run with branches off of the celiac trunk and superior and inferior mesenteric arteries empty into the portal system. The diagram on the right shows these veins coming together—some going into the splenic vein, some going into the superior mesenteric vein, and then the two coming together to form the hepatic portal vein to enter the liver.
Now running with the hepatic portal vein is the hepatic artery, which brings blood flow to the cells there, and along with that, is the bile duct containing bile that is reduced by the liver. The portal vein, hepatic artery, and the bile duct form what is known as the hepatic triad.

Pelvic Diaphragm
The caudal end of the bony pelvis is closed off by a group of muscles. One of these muscles posteriorly is the piriformis. Anterior to the piriformis is the pelvic diaphragm.
The pelvic diaphragm consists of the coccygeus muscle and the levator ani. And the levator ani consists of the pubococcygeus, the iliococcygeus, and the puborectalis. On both sides of the pelvic diaphragm are the internal obturator muscles.
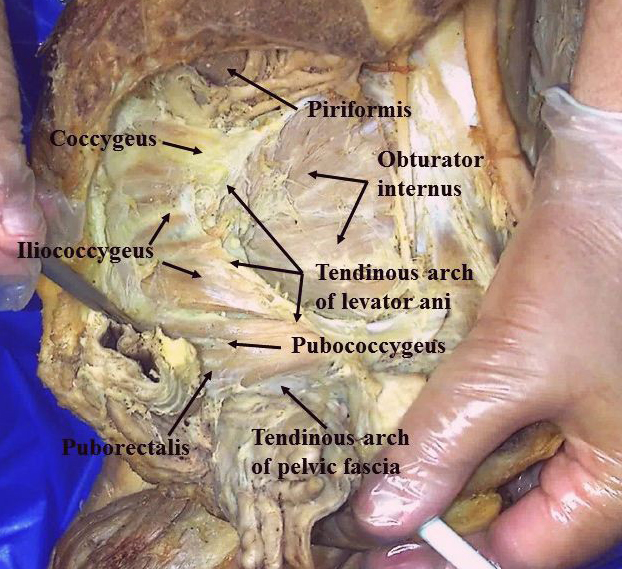
Pelvic Floor Dissection
This is a dissection of the lateral aspect of the pelvis showing the muscles in this region. At the top, you can see the piriformis and the nerves and arteries that cross it. Below that is the obturator internus. And then, to your left, is the pelvic diaphragm, beginning at the top with the coccygeus, then the iliococcygeus, and then the pubococcygeus and the puborectalis. Remember that the iliococcygeus, pubococcygeus, and puborectalis are part of the levator ani group.
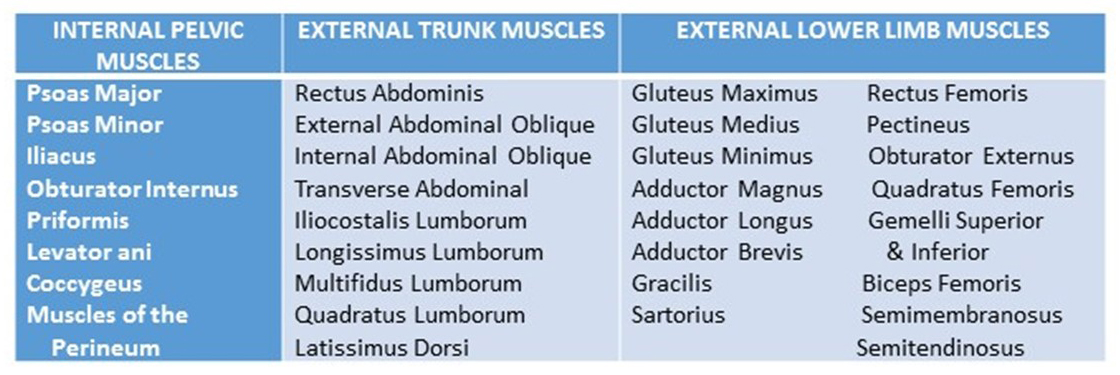
Pelvis Muscles
This table shows the muscles associated with the bony pelvis. There are muscles that lie within the pelvis, such as the pelvic diaphragm and the obturator internus. But there are also other muscles that attach to the pelvis. As you can see, there are a number of muscles from the trunk, as well as muscles from the lower extremity.
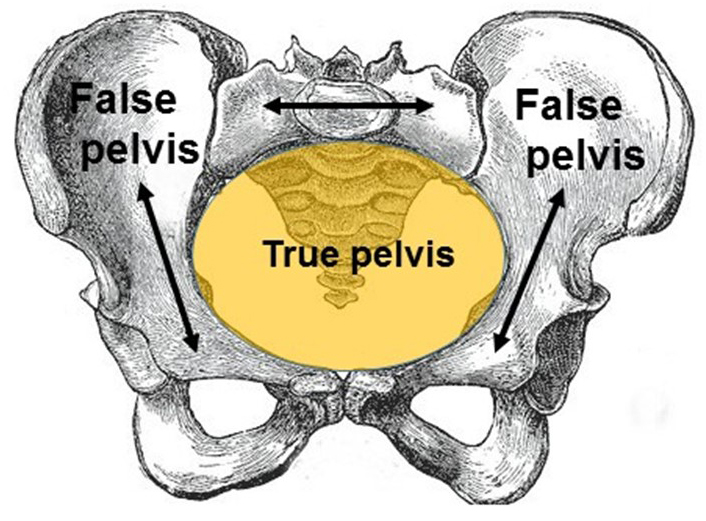
True-False Pelvis
The bony pelvis can be divided into a false pelvis and a true pelvis. The false pelvis lies between the iliac fossas of the iliac bone and contains small intestine and large intestines. The true pelvis lies caudal to the false pelvis, between the pubic bone and the ischium. It contains the bladder and reproductive organs.
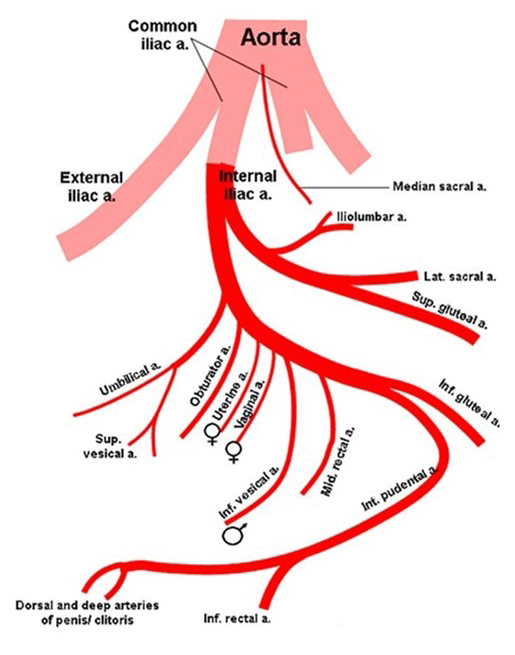
Pelvic Arteries
This diagram shows the arteries that are found in the pelvis. Off of the aorta come these common iliac arteries. Each common iliac divides into an external iliac and internal iliac.
The external iliac runs through the pelvis on its way to become the femoral artery of the lower limb. The internal iliac gives off two major divisions. One is a posterior division from which arise the iliolumbar artery, lateral sacral artery, and superior gluteal artery. The anterior division begins by giving off an umbilical artery and, from that, the superior vesicle artery to the top of the bladder. The next artery offers the obturator, which runs into the medial aspect of the thigh.
Then, in the female, there's a uterine and vaginal artery. And then, in the male there, is the inferior vesical artery going into the seminal vesicles and prostate. Both male and female have a middle rectal artery going to their rectum, an inferior gluteal artery, and an internal pudendal artery. The internal pudendal artery is the main artery going to the perineum, which we'll talk about in the next unit.
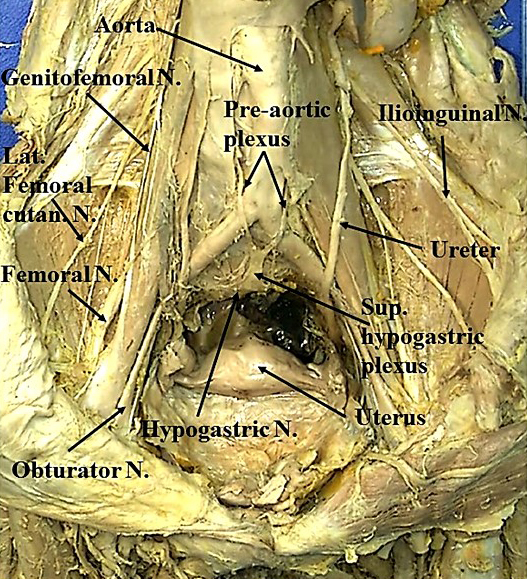
Pelvic Nerve Dissection
In this dissection of a female pelvis, you can see the route and the location of the nerves from the lumbar plexus as they cross through the pelvis. On your left, you'll see the genitofemoral nerve, lateral femoral cutaneous nerve, the femoral nerve, and the obturator nerve. On the right is the ilioinguinal nerve.
Centrally, there is the aorta, and running along the aorta—near where it bifurcates into common iliac arteries—is the preaorta plexus of the autonomics. And then, just below that, is the superior hypogastric plexus, giving off the hypogastric nerves of the autonomic system.
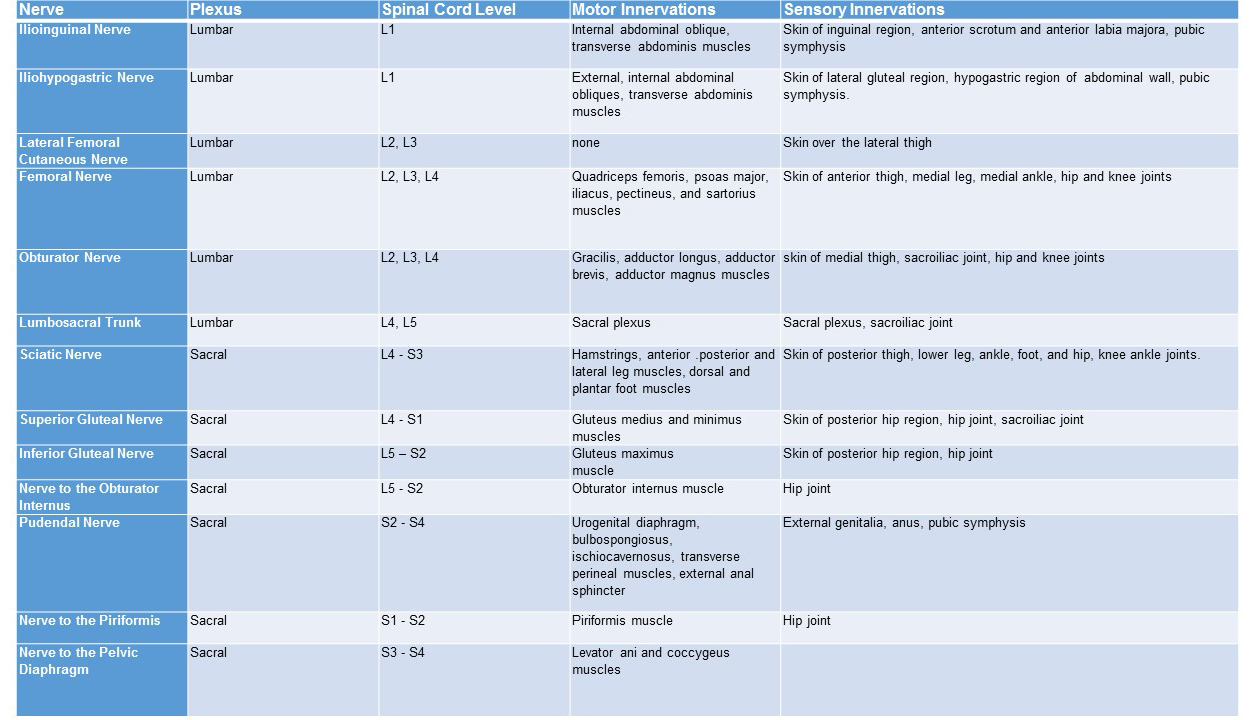
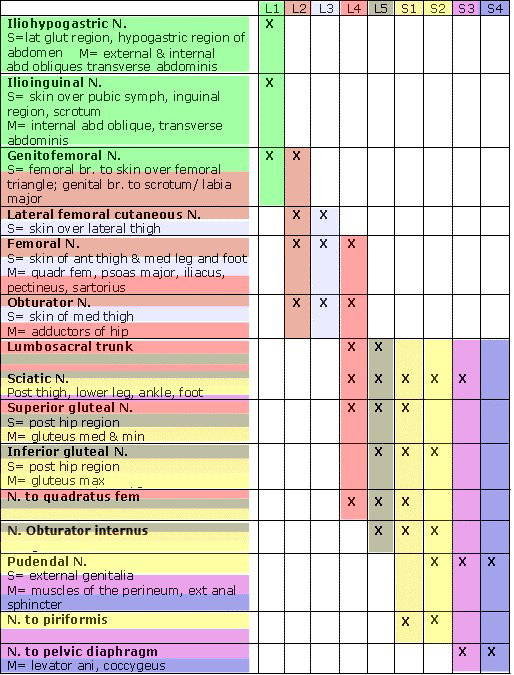
Pelvic Nerves
This is a table showing the nerves of the lumbar and sacral plexuses. For each nerve, the spinal cord level is given and the motor and sensory innervations shown. Of all these nerves, only the iliohypogastric nerve from the lumbar plexus is not found lying somewhere in the pelvis. Because there are so many nerves in the pelvis, any inflammation or damage or trauma to the pelvis can affect any of these nerves, thus making the diagnosis and treatment of pelvic problems very challenging.
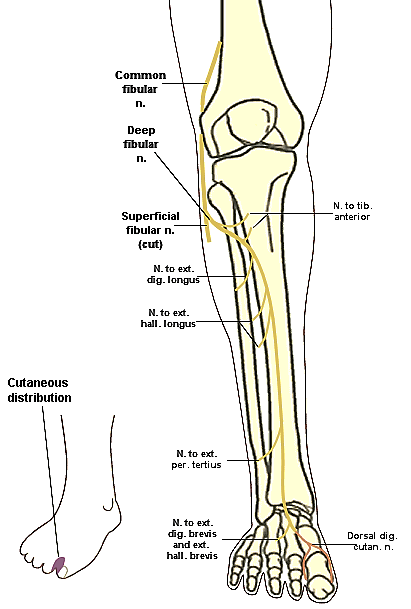
Deep Fibular Nerve
This is a diagram of the deep fibular nerve, which is a branch off the common fibular nerve, which is in the popliteal fossa. Damage to the common fibular nerve will also affect the deep fibular nerve. If the deep fibular nerve is damaged at the knee, it will affect muscles of the anterior compartment of the leg, as well as the muscles on the dorsum of the foot and the sensation between the big toe and the little toe. If the deep fibular nerve is damaged at the ankle, it will affect only muscles on the dorsum of the foot and the sensation to the area between the big toe and the little toe.
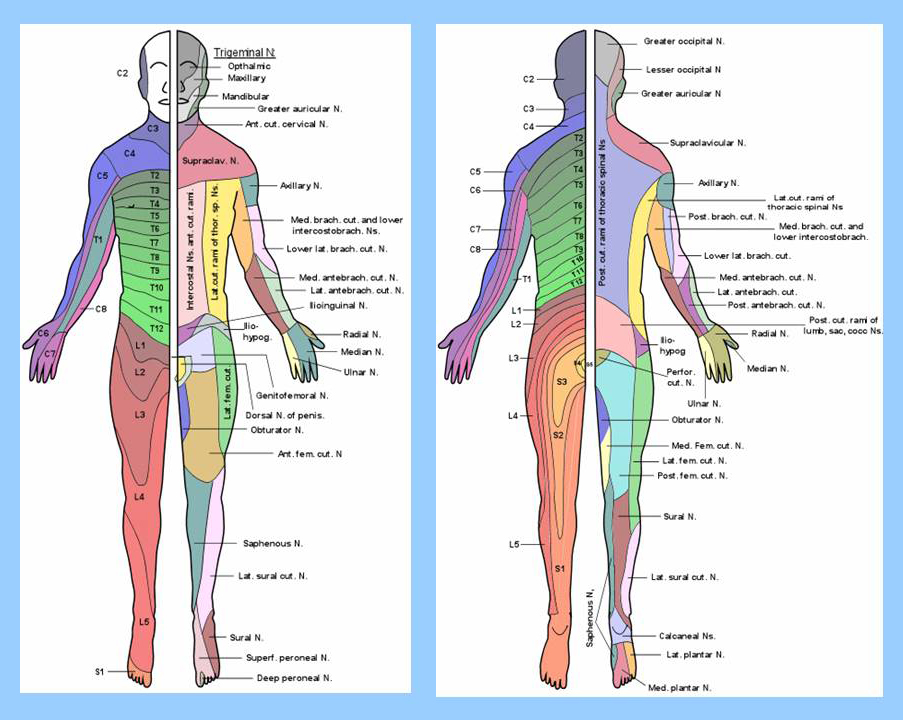
Dermatome Chart
This is a dermatome chart showing the sensorary distribution to the body. The left figure is a frontal view. The right figure is from the back.
Each figure has, on one side, the spinal nerves associated with sensation in that area and, on the opposite side, the peripheral nerves corresponding to that area. As you can see, there is quite a difference between the two. For example, in the frontal view on the left, the L3 spinal nerve overlaps with nerves from the obturator, the anterior femoral cutaneous nerve, and the lateral femoral cutaneous nerve. We see that L4 in the leg corresponds with the saphenous nerve from the femoral and the lateral sural cutaneous, which is off the common fibular. So again we see this mixture.
On the posterior view, we find that while the posterior leg is mainly going to be from the sacral plexus, the anterior leg was from the lumbar plexus. We have, near the gluteal region, S3 and S2—again overlapping the posterior femoral cutaneous nerve off of the sciatic. And then, the bottom is as one, which overlaps the sural nerve and the lateral sural cutaneous nerve, off of the common fibular nerve. So, it's important that we take into consideration not only the spinal nerve level but also the cutaneous nerve, going to that area, when we're doing our assessment of the patient.
Femoral Nerve
This is a diagram of the femoral nerve, and you can see that it has branches from the spinal nerve going into the pelvis. So, if the spinal nerve is the site of lesion, then the muscles associated with the femoral nerve in the pelvis and in the anterior thigh are going to be affected. However, if the lesion is in the anterior thigh, then the muscles of the thigh and sensation to the thigh will be affected and not the muscles of the pelvis.
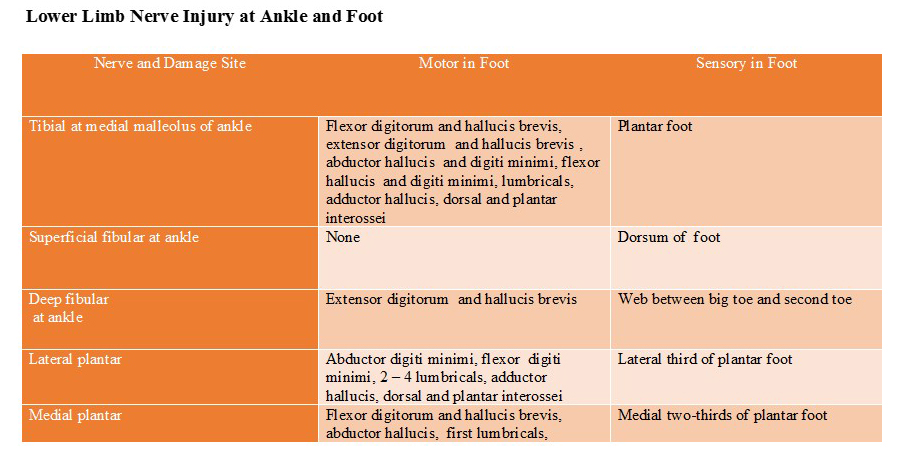
LE Injury Ankle Foot
This table shows the motor and sensory effects in the foot when there is damage to the tibial nerve at the ankle; superficial nerve and deep fibular nerve at the ankle; and the medial and lateral plantar nerves. Compare the motor and sensorary effects of an injury to the tibial nerve at the ankle and the medial and lateral plantar nerve injuries in the foot. Also, compare the sensorary effects of an injury to the superficial and deep fibular nerves at the ankle.
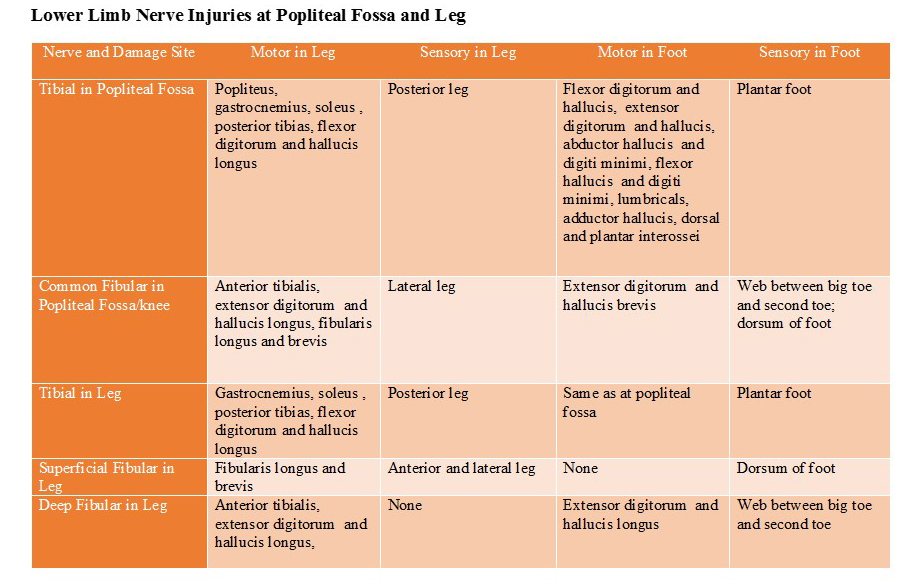
LE Injury Popliteal Fossa and Leg
This table shows the motor and sensuary structures in the leg and the foot that are affected by injury to the tibial and common fibular nerves in the area of the popliteal fossa and the tibial, superficial, fibular, and deep fibular nerves in the leg. Compare the tibial nerve injury at the popliteal fossa with the leg and the common fibular injury at the popliteal fossa with the superficial and deep fibular nerves.
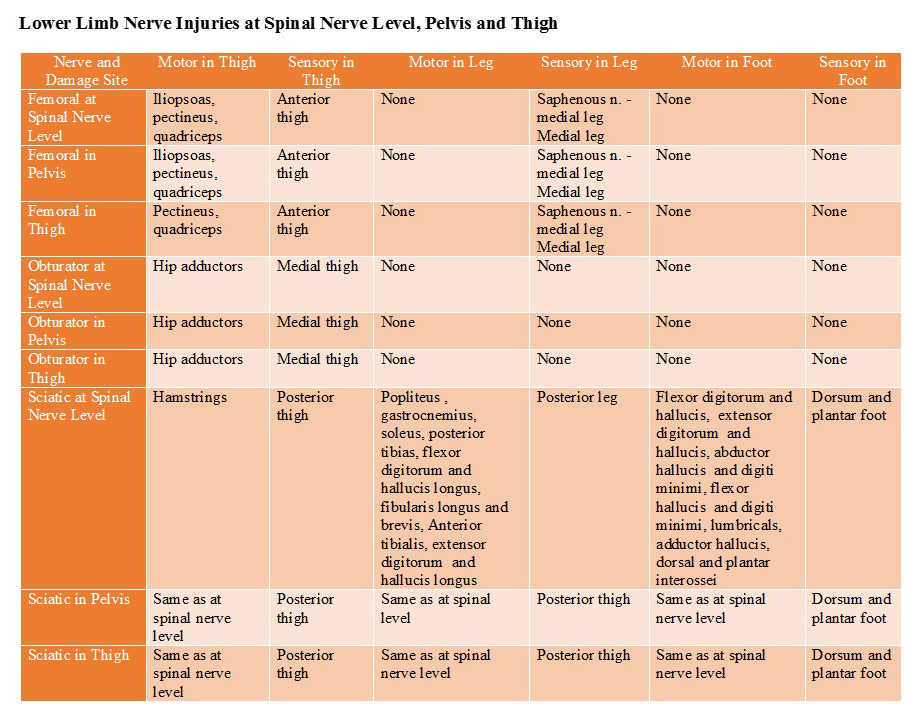
LE Injury Spinal Nerve, Pelvis, Thigh
This table shows the results of lesions of the femoral, obturator, and sciatic nerve at the level of the spinal nerve, in the pelvis, and in the thigh. Note and compare the similarities and differences in motor and sensorary involvement for all three nerves at each level of lesion.
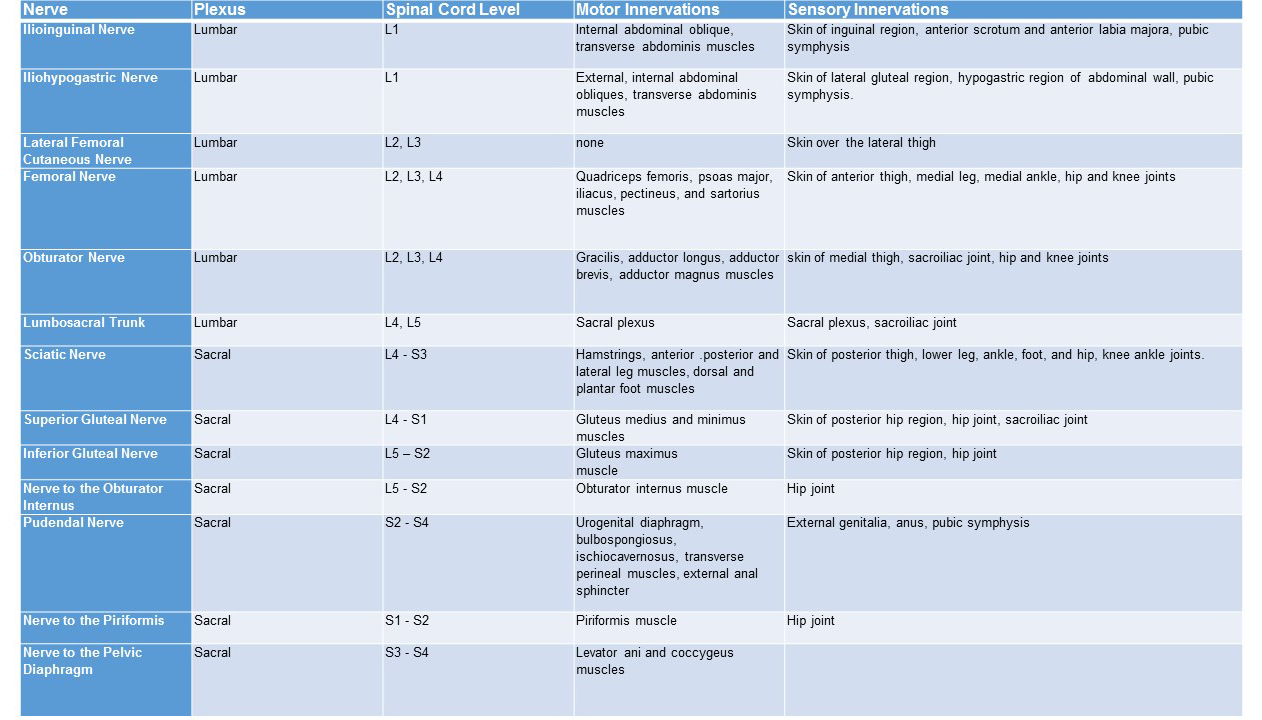
LE Nerves
This chart shows the nerves of the lumbar and sacral plexuses, their spinal cord levels, and descriptions of their overall sensory and motor innervation. However, the lesions to these nerves can occur different levels. For example, the femoral nerve lesion can occur at the spinal nerve, in the pelvis, or in the thigh. For the sciatic nerve, nerve damage can also occur at the spinal nerve level, the pelvis, and the posterior thigh. But because the sciatic has branches that go to the leg and the foot, it really depends on whether that lesion is of the sciatic or if the lesion is associated with these terminal branches.
Lumbar Sacral Nerve Chart
Nerves to the lower limb arise from the lumbar plexus and sacral plexus. In this chart, the nerves of the lumbar plexus and a brief description of their sensory and motor components are at the top of the chart, and the sacral plexus is at the bottom. The nerves to the lower extremity can be affected at several levels, and one of these is at the spinal nerve.
In this chart, we see the spinal nerve distributions for the different nerves of the lumbar and sacral plexuses. Notice that the spinal nerve contributes to multiple nerves in the lumbar and sacral plexus. For example, L2 goes to the lateral femoral cutaneous, which is lateral sensation to the thigh, as well as to the femoral and obturator nerves.
L4 goes to the femoral and obturator nerves of the lumbar plexus, as well as the superior gluteal and the sciatic nerve and the nerves of the quadratus lumborum of the sacral plexus. And, L5 goes to the sciatic, superior gluteal, inferior gluteal, and nerves of the quadratus lumborum and obturator internus. So, you can see that a spinal nerve lesion can have effects in multiple areas of the lower limb.
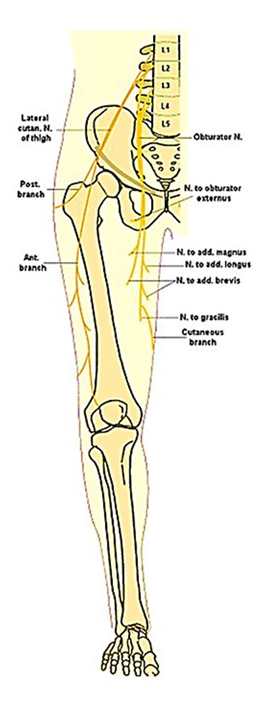
Obturator Nerve
This is a diagram of the obturator nerve from the lumbar plexus. It, like the femoral nerve, arises from L2 to L4 spinal nerves. It also goes into the pelvis and then into the leg. However, a lesion of the spinal nerve or the obturator nerve in the pelvis or in the leg end up with the same results, affecting the adductors and the sensation to the medial thigh.
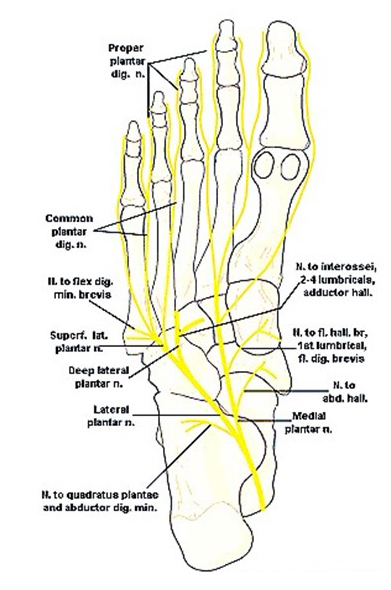
Plantar Nerves
This is a diagram of the plantar nerves of the foot. The medial and lateral plantar are both branches off of the tibial nerve, and so they are affected if the tibial nerve is damaged in the popliteal fossa, posterior leg, or at the ankle. Damage to the tibial nerve affects both the medial and lateral plantar nerve. Involvement of the medial plantar nerves affects the muscles associated with the big toe and sensation along the medial plantar surface of the foot. Involvement of the lateral plantar nerve affects the muscles on the lateral side and central portions of the foot and sensation to the lateral two thirds of the plantar surface of the foot.
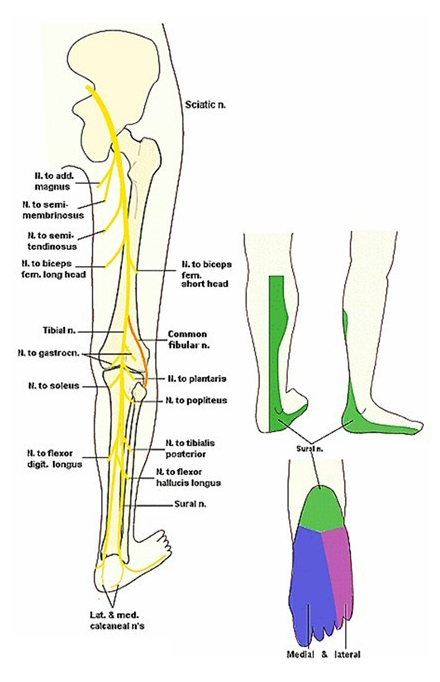
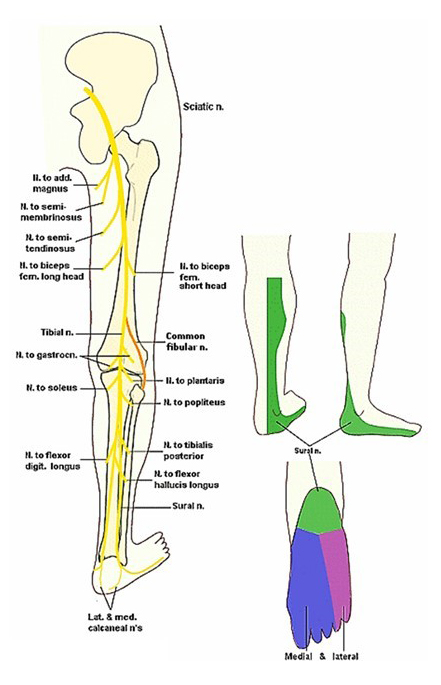
Sciatic Nerve
This is a diagram of the sciatic nerve. The nerve arises from the ventral rami of L4 through S3. Like the femoral and obturator nerves, it runs in the pelvis. And then it goes posteriorly into the posterior thigh. From the posterior thigh, it goes to the knee, where it divides into its two main components—the tibial nerve and the common fibular nerve.
In the case of the sciatic nerve, the location of the lesion is important. If the lesion is at the spinal nerve, then it will affect structures at the pelvis and through the entire lower limb. If the lesion is in the posterior thigh, then it will affect the muscles and sensation in the posterior thigh and down into the leg and the foot but not the structures innervated in the pelvis. If the lesion is at the level of the knee, then it will affect structures in the leg and foot but not structures in the thigh and pelvis.
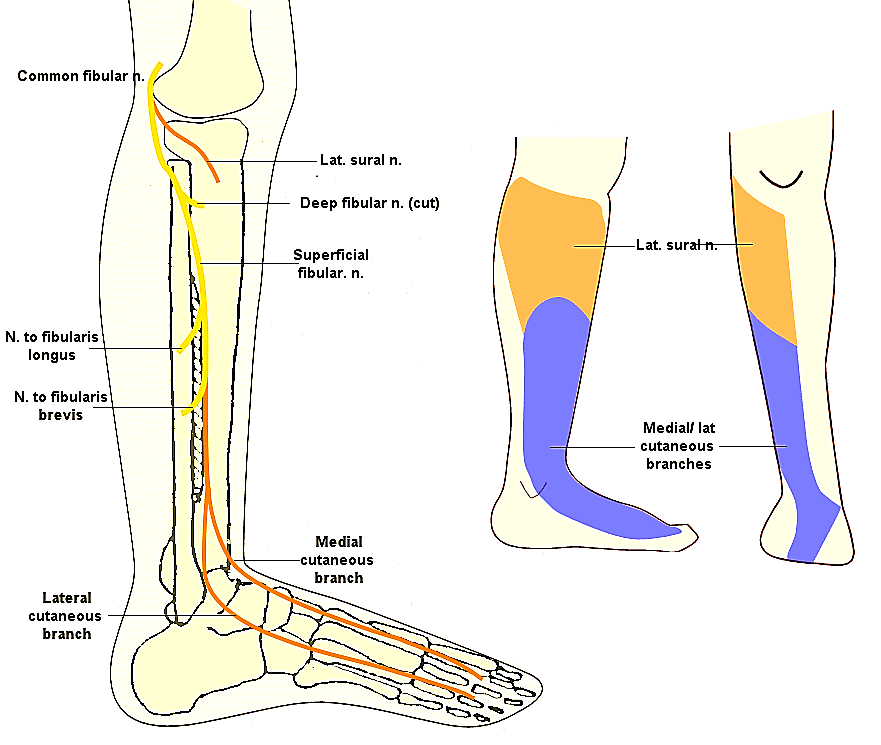
Superficial Fibular Nerve
This is a diagram of the superficial fibular nerve, which is a branch also off of the common fibular nerve. If the common fibular nerve is damaged, it will affect both the deep fibular nerve and the superficial fibular nerve. Damage to the superficial fibular nerve affects the muscles of the lateral compartment of the leg, as well as the sensation to the lateral leg and most of the top of the foot. Damage to the superficial fibular nerve at the ankle only affects the sensation to the dorsum of the foot.
Tibial Nerve
This is a diagram of the tibial nerve arising from the sciatic nerve in the area of the popliteal fossa. The tibial nerve runs down the posterior leg and under the medial malleolus and into the bottom of the foot. Damage to the tibial nerve at the popliteal fossa results in involvement of the muscles of the posterior compartment of the leg, as well as the muscles at the plantar surface of the foot. This damage also affects sensation to the posterior leg and sensation to the plantar foot. The tibial nerve can also be damaged at the ankle. If this occurs, then the posterior leg muscles are uninvolved but the muscles and sensation to the plantar surface of the foot are involved.
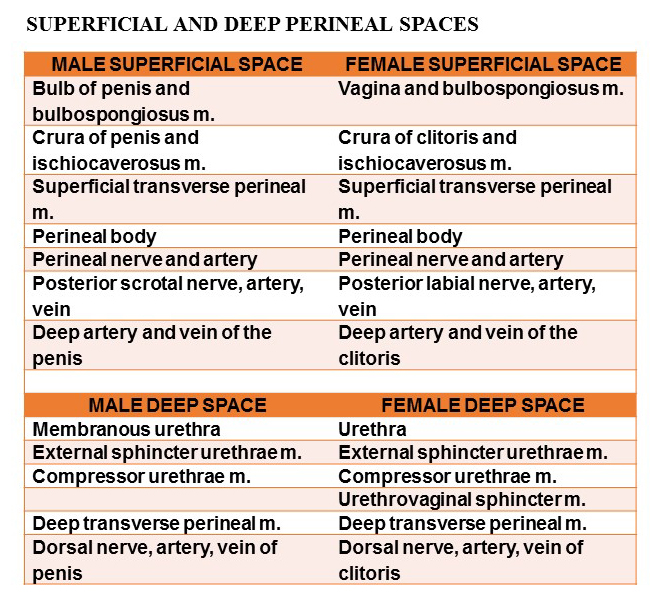
Male & Female Perineal Contents
This table shows the contents of the male and female superficial perineal space and deep perineal space. Notice that the contents are very similar between males and females.
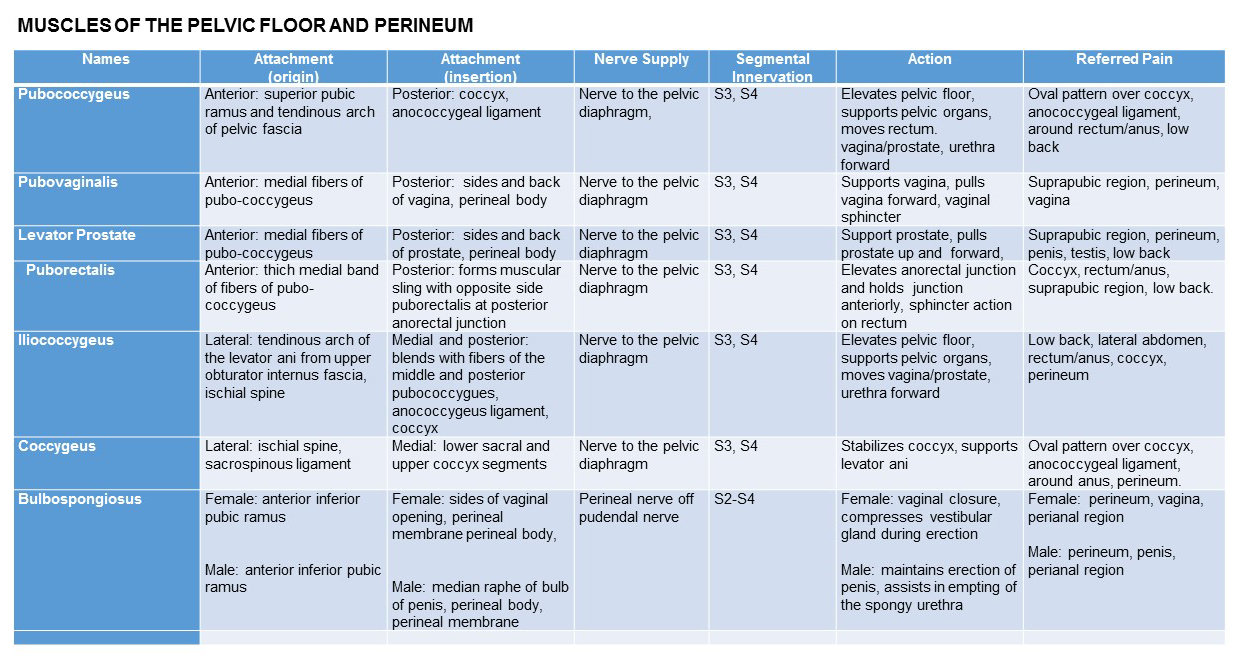
Muscles of Pelvic Floor 1
This table and the next table summarize the muscles of the pelvic floor and perineum. In this table, we see the muscles forming the pelvic diaphragm—the pubococcygeus, the puborectalis, the iliococcygeus, and the coccygeus.
The pubovaginalis and the levator prostates are branches off of the pubococcygeus—one going in the female to the vagina, the other one in the male to the prostate. At the bottom is a muscle called the bulbospongiosus, which we find in the superficial perineal space.
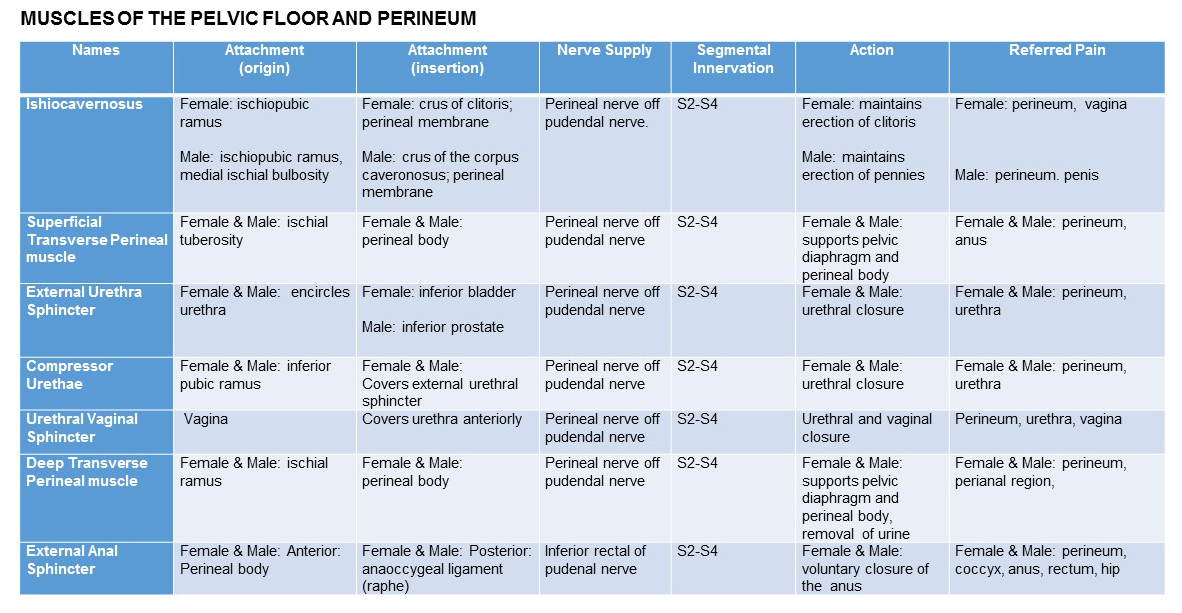
Muscles of Pelvic Floor 2
This second table shows the muscles of the pelvic floor and perineum. You start at the top with the ischiocavernosus and superficial transverse perineal muscle, which are both found in the superficial space of the urogenital triangle.
The external urethral sphincter wraps around the urethra in both the male and female. And in the male, the urogenital diaphragm consists of the compressor urethra and the deep transverse perineal muscle. In the female, the urogenital diaphragm consists of the compressor urethrae, the urethral vaginal sphincter, and the deep transverse perineal muscle. In the anal triangle is the external anal sphincter.
Perineum Borders
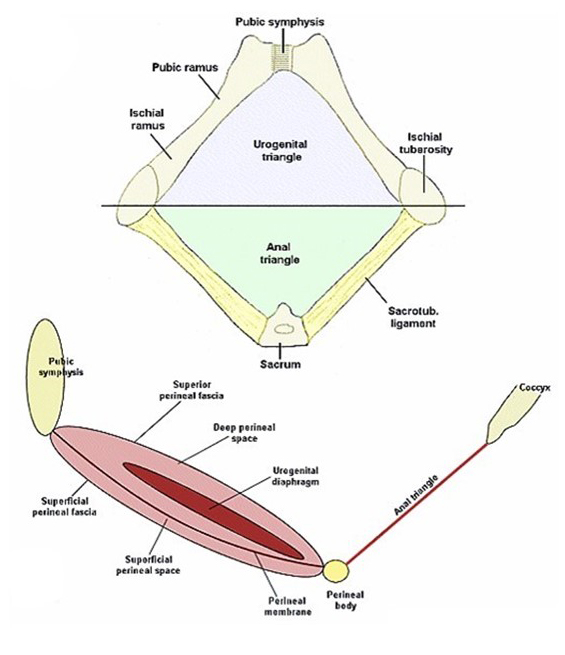
The top diagram shows the borders of the diamond shape perineum. Anteriorly is the pubic symphysis, on each side, the pubic ramus and ischial ramus. In the back is the sacrotuberous ligament to the sacrum.
This diamond shaped region is divided into two triangles. The urogential triangle and the anal triangle. In the bottom view of this diagram, you see a sagittal section to the area of the perineum.
On your left is the pubus, on the right is the coccyx, and down the center is a fiber structure known as the perineal body. The left side of this area is the urogential triangle, the right side is the anal triangle.
The urogential triangle is divided into two spaces by a membrane known as the perineal membrane. In the superficial space are parts of the external genitalia and muscle. And in the deep space lies the urogenital diaphragm.
Remember that in the unit on the bony pelvis, we talked about the pelvic diaphragm. This is the urogenital diaphragm. Don't confuse them.
Perineum Nerves & Arteries
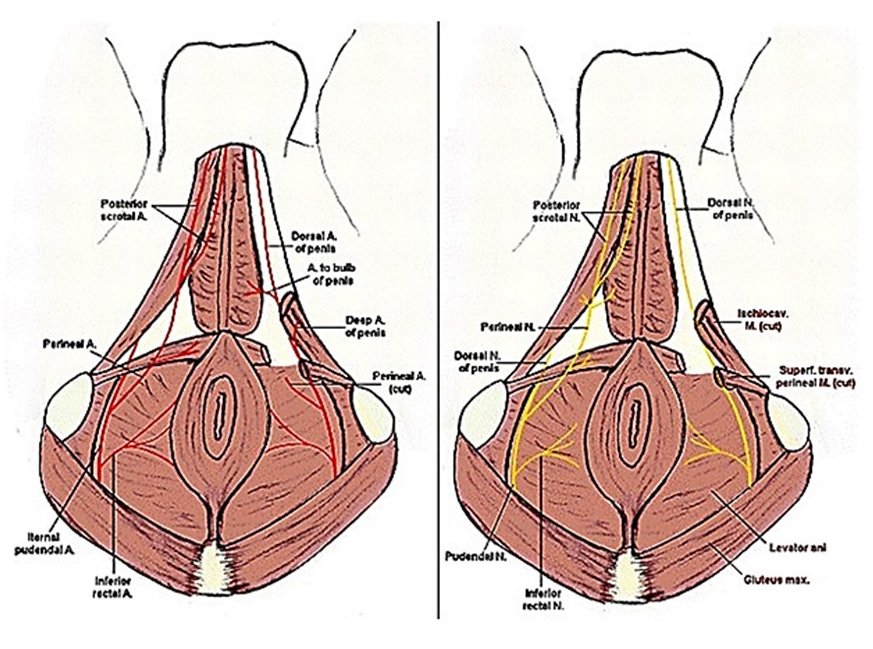
This diagram shows the arteries on the left of the perineum and, on the right, the nerves of the perineum. The main artery coming into the perineum is the internal pudendal artery, which gives off an inferior rectal artery to the area of the anus in the anal triangle. It then divides into a perineal artery, which gives off a posterior scrotal or labeal majora artery, and a deep artery to the clitoris or penis.
The nerve to this area is the pudendal nerve, which likewise gives off an inferior rectal nerve going to the area of the external anal sphincter, and then divides into a perineal nerve and a dorsal nerve to the penis or clitoris.
The perineal nerve ends at the posterior scrotal nerve, or posterior nerve, to the labia majora. Damage to the pudendal nerve will result in anal and urinary incontinence, while damage to only the perineal nerve will result in only urinary incontinence and no anal incontinence.
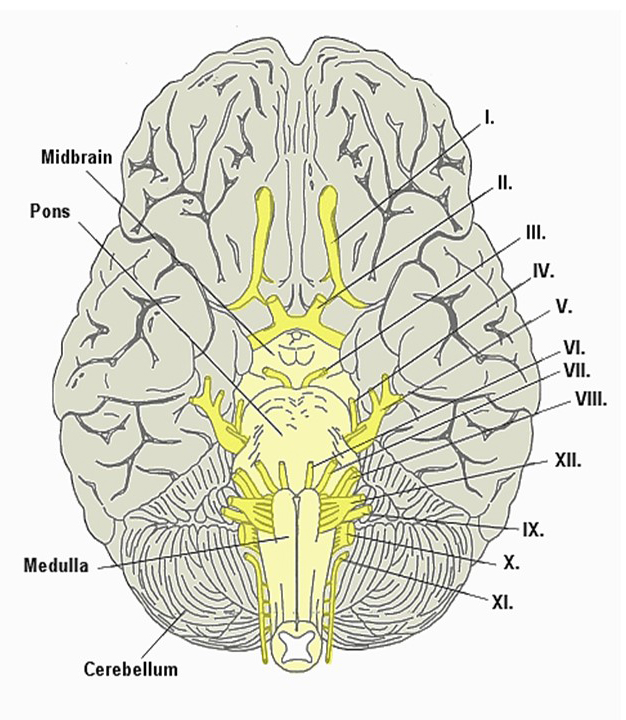
Brain Cranial Nerves
This is a drawing of the base of the brain, showing the location of the 12 cranial nerves. You should be able to identify each of the cranial nerves by their Roman numeral.
Cranial Nerve Table
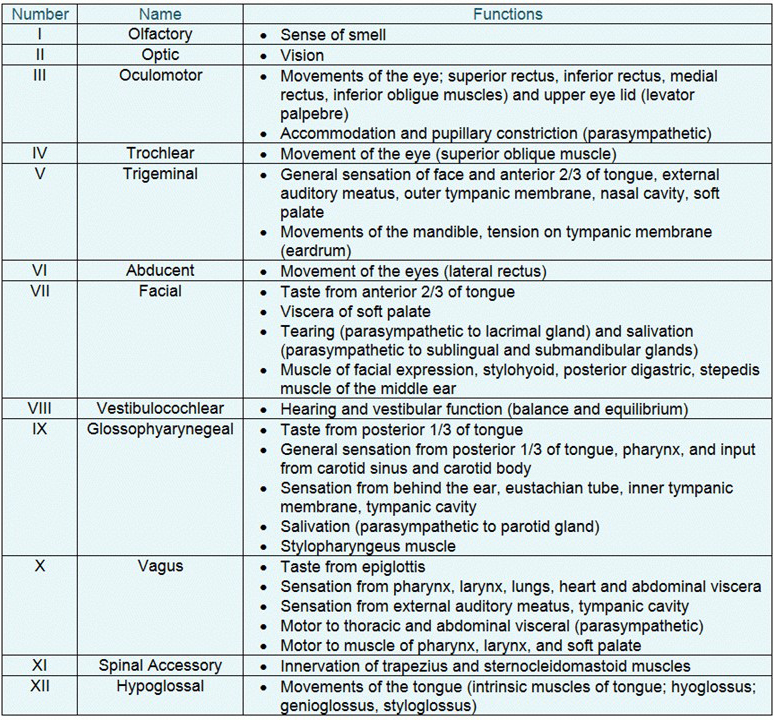
This table gives the Roman numeral, name, and function of the 12 cranial nerves.
Trigeminal Nerve
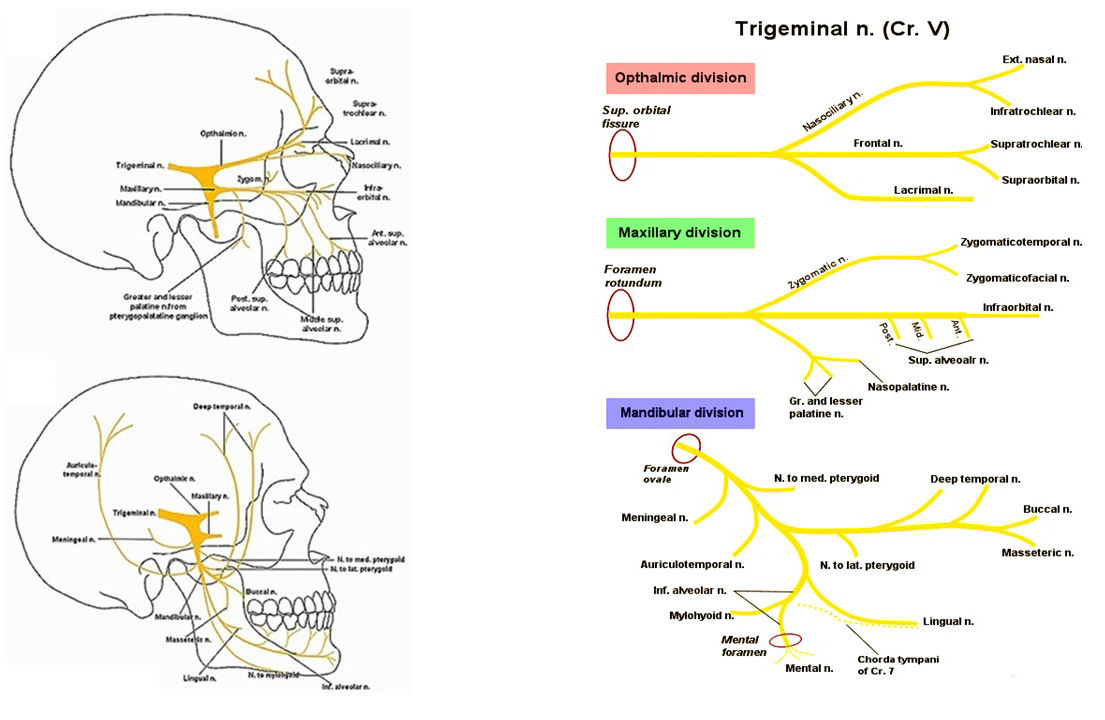
These diagrams show the branches of the trigeminal nerve. On the left, the branches of the ophthalmic division and the maxillary division are superimposed on the skull. Notice that the ophthalmic branches tend to concentrate in the area around the eye, while the branches of the maxillary division go to the palate, upper teeth, and just below the orbit.
In the lower-left diagram is the mandibular division of the trigeminal nerve. This is the only part of the trigeminal system that has motor fibers. The motor fibers here go to the muscles of mastication, temporalis, masseter, medial and lateral pterygoids, as well as sensation to the teeth and to the tongue and also to parts of the side of the jaw and the front part of the jaw.
On the right-hand side are line drawings of each of the three divisions of the trigeminal. At the top is the ophthalmic division, with its branches going, again, primarily around the orbit in the supratrochlear, supraorbital, and infratrochlear regions. The maxillary division below shows the branches going to the hard and soft palate, also, the upper teeth, and sensory parts going over the area of the zygomatic arch and below the eye.
The mandibular division has its branches going to the medial and lateral pterygoid, temporalis, and masseter. The buccal branch. The auriculotemporal sensory branch is going to the area of the lateral jaw and the cheek area. The infraorbital nerve is sensory to the lower teeth and motor to the mylohyoid muscle and the anterior digastric. The lingual is the sensory nerve to the anterior two-thirds of the tongue.
Notice that running with lingual nerve is the chorda tympani. The chorda tympani is a branch of the facial nerve, which runs with the lingual nerve to provide taste to the anterior 2/3 of the tongue.
Tongue
The tongue consists of intrinsic and extrinsic skeletal muscles. The intrinsic skeletal muscle makes up the body of the tongue itself, and the extrinsic muscles are those that move the tongue in different directions.
The prime extrinsic muscles of the tongue are the genioglossus, the hyoglossus, and the styloglossus. The intrinsic and extrinsic muscles of the tongue are innervated by the hypoglossal nerve.
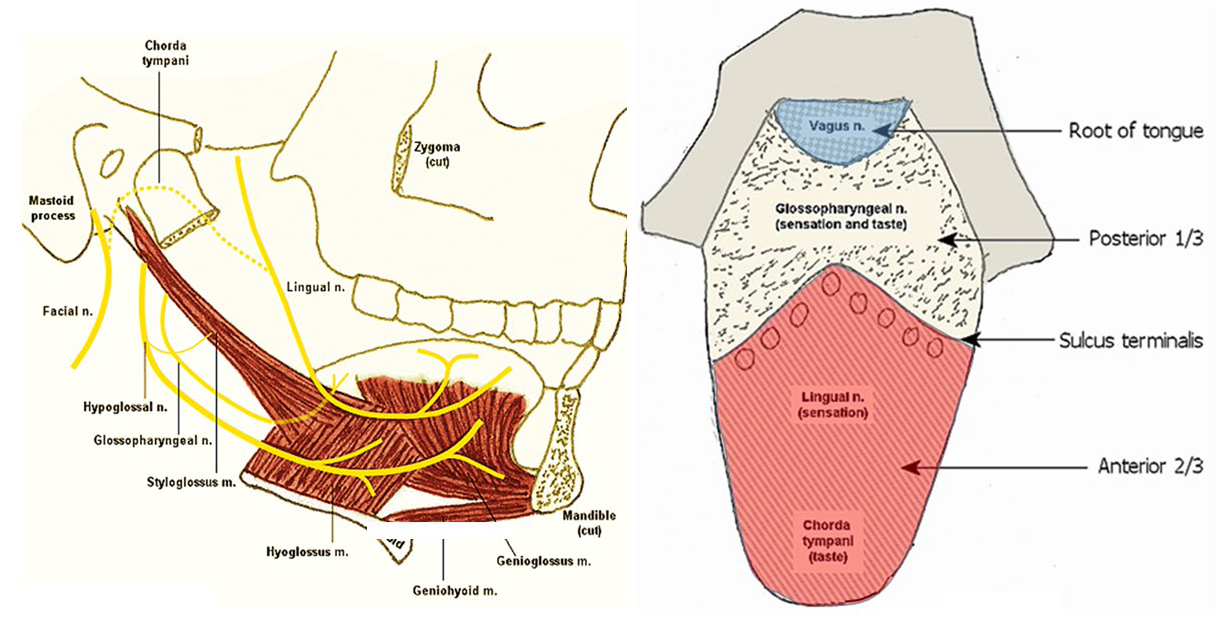
In the diagram on the left, you can see the hypoglossal nerve coming in to the tongue to innervate these muscles as well as the muscles of the tongue. In addition, we see the glossopharyngeal nerve, which is a sensory nerve to the tongue, and the lingual nerve, which is also a sensory nerve to the tongue.
Coming from the area of the ear is the chorda tympani. This nerve is from the facial nerve and runs with the lingual nerve to provide taste from the anterior two-thirds of the tongue.
On the right is a drawing showing the sensory components of the tongue. The anterior two-thirds of the tongue has general sensation from the lingual nerve off the trigeminal, and taste is via the chorda tympani off the facial. The glossopharyngeal nerve provides general sensation and taste to the posterior third of the tongue, which is sometimes referred to as the lingual tonsil.
The root of the tongue is innervated by the vagus nerve. You may recall that the vagus nerve also innervates the esophagus and the intestines. This is why, when you stimulate the root of the tongue, that you may activate the smooth muscle of the stomach and the intestines.
Temporomandibular Joint
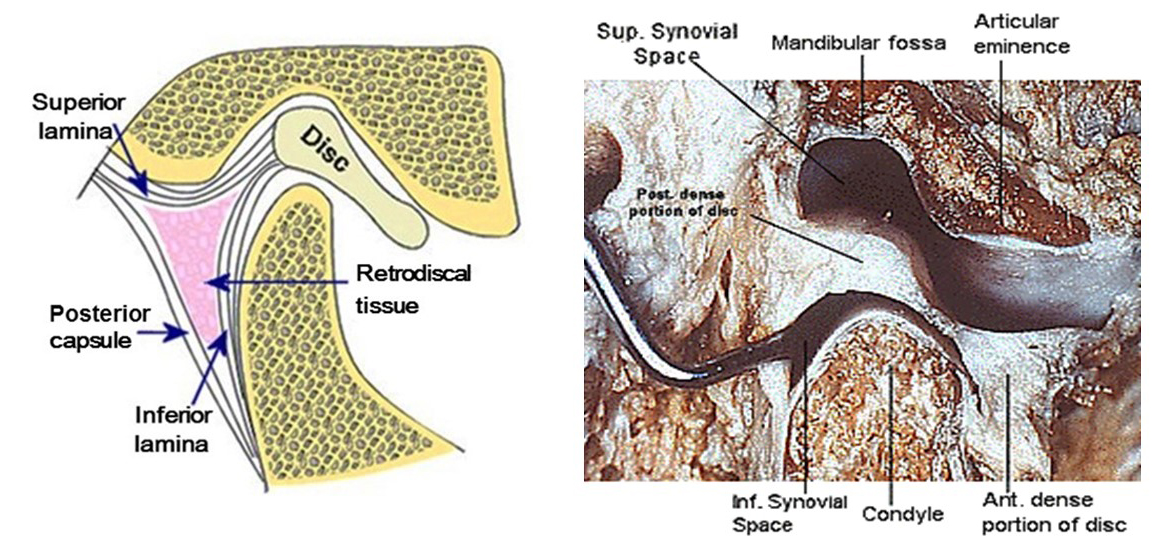
On the left is a diagram of the temperomandibular joint, and on the right is a dissection of this joint, showing the mandibular condyle the mandibular fossa and the inter articular disc. The diagram on the left also shows two important lamina—the superior lamina, which is elastic, and the inferior lamina, which is fibrous.
As the disc moves forward during jaw opening, the superior lamina stretches and the inferior lamina tightens to restrict this movement. As the disc then recoils during closing, the superior lamina recoils, bringing the disc backward. Attached to the front part of the joint capsule is a muscle called the lateral pterygoid muscle, which controls the return of the disc back to its normal position with the jaw closed.
Palate
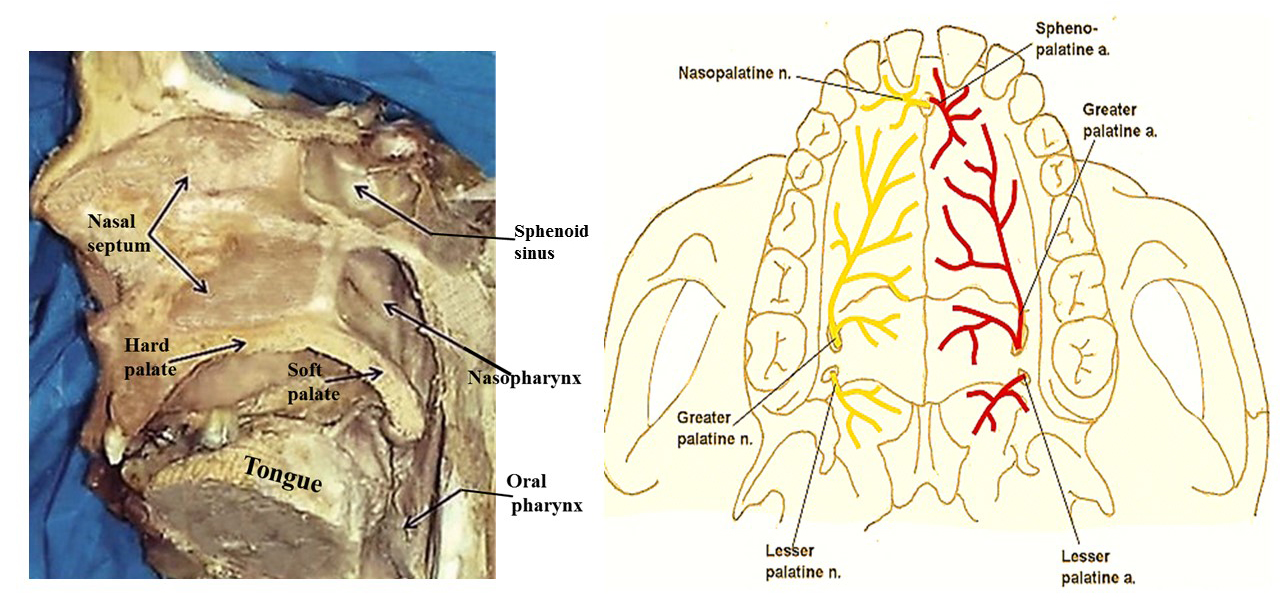
On the left is a dissection of the oral cavity showing the hard palate, soft palate, and the tongue. On the right is a diagram showing the nerve and arterial blood supply to the hard and soft palate.
The nerve supply to the hard palate and soft palate is from the maxillary division of the trigeminal. And there are three branches. Up at the incisors, the innervation is by the nasopalatine nerve, the hard palate is by the greater palatine nerve, and the soft palate by the lesser palatine nerve.
On the other side are the blood supplies to the palate from the maxillary artery. Up near the incisors, the blood supply arises from the sphenopalatine artery. And for the hard palate, the blood is from the greater palatine artery; and for soft palate, the lesser palatine artery.
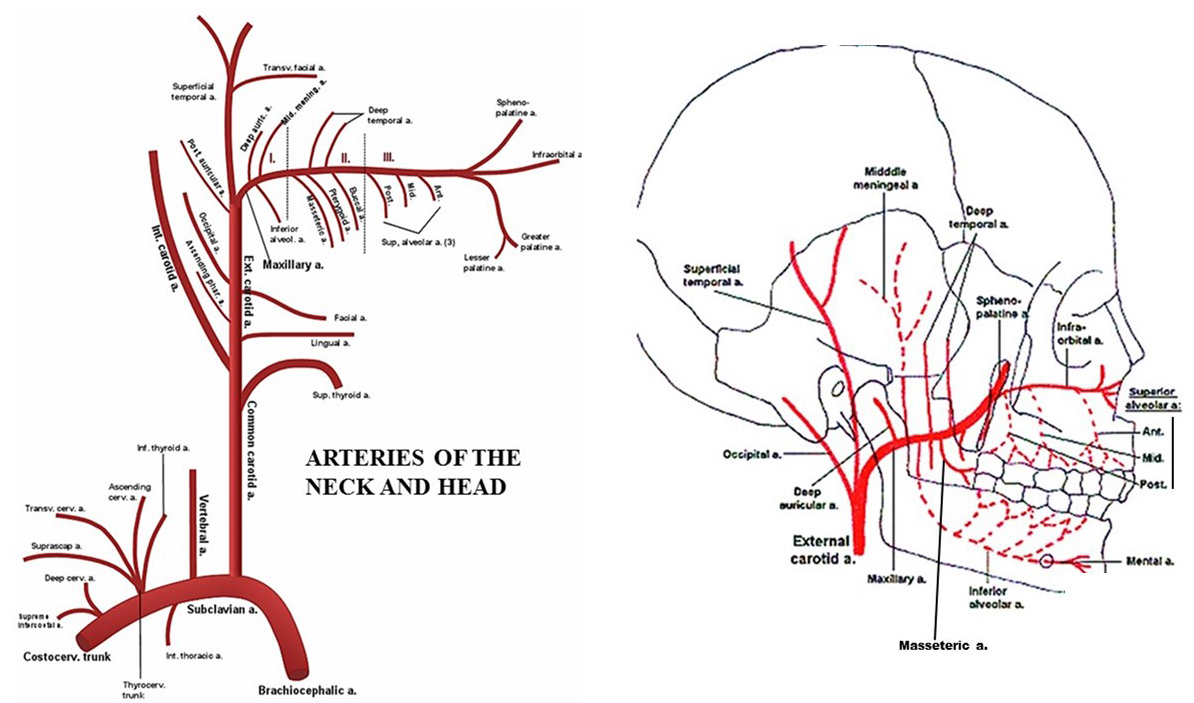
Carotid Artery
The figure on the left is a diagram of the blood supply to the head and neck. It begins off the subclavian in the root of the neck with the vertebral and branches off and thyrocervical trunk. We then proceed cranially to the common carotid, which gives off an internal carotid to the brain and the external carotid basically to the head.
Off of the external carotid, we see a superior thyroid artery, then there is the lingual to the tongue, the facial to the face region, and then, further upward, there is the maxillary and the superficial temporal. The maxillary is the main blood flow to the muscles of mastication, to the upper and lower teeth, to the palate, and even provides blood to the meninges of the brain. The maxillary is divided into three parts by the lateral pterygoid, with the second part giving rise to blood vessels to the muscles of mastication, the first part to the lower teeth, and the third part to the palate and upper teeth.
The figure on the right shows the maxillary arteries superimposed on the skull. And you can see the inferior alveolar artery going downward through the mandible and giving blood supply to the teeth. See the middle meningeal going upward to the bone meninges of the brain.
As we go anteriorly, we come to the second part of the maxillary artery, with branches to the muscles of mastication. There's a deep temporal, there's a masseter, and there are also pterygoid branches. Then we go into the third part, and here we have the branches to the upper teeth as well as the greater and lesser palatine branches to the hard and the soft palate.